
Understanding facial anatomy for injectables is the foundation of every safe, natural-looking cosmetic treatment. The face is not a flat canvas. It is a layered, three-dimensional structure made up of skin, fat compartments, muscle, ligaments, nerves, blood vessels, and bone, each playing a distinct role in how you look and how injectables behave once placed. When a practitioner understands these layers precisely, treatments like Botox and dermal fillers produce balanced, harmonious results. When that knowledge is absent, the risks range from visible lumps and asymmetry to serious complications like vascular occlusion. Knowing what your injector should understand, and why, puts you in a far stronger position as a patient.
What are the key anatomical layers involved in facial injectables?
Facial anatomy consists of five layers: skin, hypodermis (subcutaneous fat), the superficial musculoaponeurotic system (SMAS), deep fat compartments, and the periosteum with underlying bone. Each layer has a different density, mobility, and vascular supply, which directly determines where a product should be placed and what type of filler is appropriate. Injecting at the wrong depth in the wrong zone is one of the most common causes of unnatural results.
The table below outlines the five layers, typical injection depths, and the associated clinical considerations:
| Layer | Typical injection depth | Key considerations |
|---|---|---|
| Skin (dermis) | Superficial, intradermal | Fine lines, superficial hydration; risk of visible product |
| Hypodermis (subcutaneous fat) | Subcutaneous | Volume, contouring; variable fat thickness by region |
| SMAS | Mid-depth | Structural support; avoid disrupting muscle planes |
| Deep fat compartments | Deep, supraperiosteal | Volume restoration; supports bony framework |
| Periosteum and bone | Supraperiosteal | Structural anchoring; safest plane for deep volumisers |
The distinct fat compartments of the face are particularly relevant to injectable anatomy basics. The medial cheek fat, nasolabial fat, and deep medial cheek fat each deflate and descend at different rates with age. A practitioner who understands these compartments can restore volume where it has genuinely been lost, rather than simply adding product where a fold is visible. Supraperiosteal placement on bone provides structural support and avoids the superficial puffiness that gives an overfilled appearance.
Nerves and arteries run through and between these layers in predictable but variable paths. The facial nerve branches, the temporal artery, the angular artery, and the infraorbital artery are the structures most relevant to injectable safety. Knowing their approximate locations relative to bony landmarks is what separates a technically sound treatment from a dangerous one.

Pro Tip: Ask your practitioner which layer they are targeting and why. A confident, anatomy-trained injector will answer this without hesitation.
Which facial areas carry the highest risk during injectable treatments?
Certain regions of the face are considered high-risk zones because critical arteries and nerve branches run close to the surface or converge at predictable points. The glabella (between the brows), the nose, the temples, the periorbital region, and the midface are the areas where complications are most likely to occur if technique is imprecise.
The primary vascular risk is arterial occlusion. If filler is inadvertently injected into or compresses an artery, blood flow to downstream tissue is interrupted. In the most serious cases, this can lead to skin necrosis or, when the ophthalmic artery is involved, permanent vision loss. High-risk zones contain critical arteries including the temporal, angular, and infraorbital arteries, all of which sit in proximity to common injection sites.
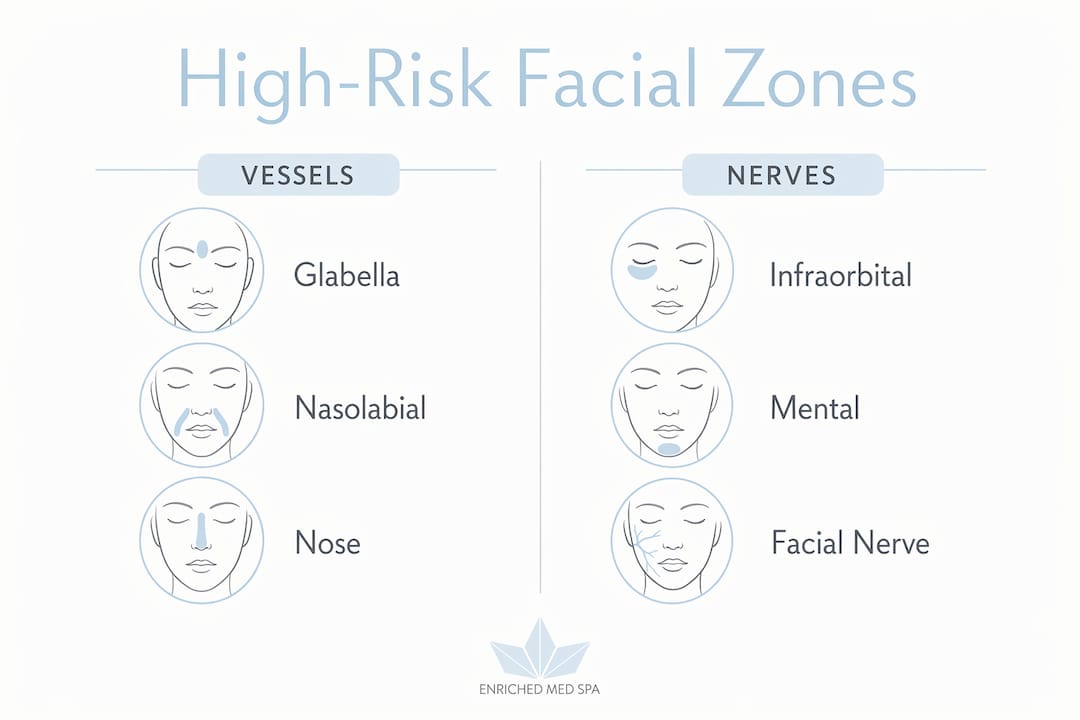
Nerve injury is a secondary but real concern. The supraorbital and supratrochlear nerves exit through foramina near the glabella. The infraorbital nerve exits just below the orbital rim. Pressure or direct trauma to these structures can cause temporary or lasting numbness and pain.
Skilled practitioners manage these risks through several evidence-based strategies:
- Using blunt-tip cannulas in high-risk zones, which displace vessels rather than puncture them, greatly minimising vascular complications
- Injecting micro-aliquots less than 0.1 mL with slow, continuous retrograde motion to limit pressure and allow precise volume control
- Aspirating before injecting in needle-based techniques, particularly near known arterial paths
- Using bony landmarks to map safe injection corridors before treatment begins
“Facial assessment includes palpating bony landmarks and evaluating muscle activity to create a 3D understanding of unique anatomy, preventing complications like vascular events.” — The importance of facial anatomy in aesthetic treatments
Pro Tip: Practitioners who perform a thorough facial mapping assessment before touching a needle or cannula are not being overly cautious. They are being appropriately trained. This step is non-negotiable in anatomy-based practice.
How does facial anatomy shape natural-looking injectable results?
Natural-looking results prioritise facial harmony and balance over filling individual lines or adding maximum volume. This is the core principle behind understanding natural-looking injectables, and it is entirely dependent on anatomical knowledge. A practitioner who treats a nasolabial fold in isolation, without considering the fat compartment deflation driving it, will often produce a result that looks corrected but not natural.
The SMAS is particularly important here. This fibromuscular layer connects the superficial muscles of facial expression to the overlying skin. Injecting too close to or within the SMAS without understanding its function can restrict natural movement, contributing to the “frozen” appearance that many patients fear. Respecting muscle planes and targeting the appropriate depth for each product preserves the dynamic expressiveness that makes a face look alive.
Achieving a natural outcome through anatomical planning follows a clear sequence:
- Assess the bony framework. Bone resorption in the midface and jawline reduces structural support, which must be addressed before adding superficial volume.
- Evaluate fat compartment volume and position. Identify which compartments have deflated or descended and target those specifically.
- Consider muscle activity. Map areas of hyperactivity (forehead, glabellar complex, perioral) where neuromodulators like Botox, Nucieva, or Xeomin are appropriate.
- Match filler rheology to the anatomical layer. Firmer, more cohesive products like Juvederm Voluma or Teosyal RHA 4 suit deep structural placement. Softer, more fluid products suit superficial refinement.
- Treat multiple regions for overall harmony. Addressing the midface, jawline, and temples together produces a more balanced result than correcting one area in isolation.
Structural planning based on bone and fat anatomy avoids the overfilled or puffy appearance that results from product placed without anatomical context. Some patients genuinely need significant volume restoration to maintain facial harmony. The goal is always to respect individual facial architecture, not to apply a standardised formula. You can read more about how this works in practice in this overview of how fillers restore natural rejuvenation.
Pro Tip: If a consultation focuses entirely on the lines you want treated rather than your overall facial structure, that is worth noting. Anatomy-based planning starts with the whole face, not a single concern.
How does aging change facial anatomy and affect injectable planning?
Aging is not a single process. It involves simultaneous changes across every facial layer, and these changes necessitate anatomical-based injectable strategies tailored to each region and patient. Understanding facial structure as it changes over time is what allows an injector to treat the cause of an aged appearance rather than just its surface expression.
The key age-related anatomical changes and their injectable implications are:
- Bone resorption: The maxilla, mandible, and orbital rim all lose volume with age, reducing the structural scaffold that supports overlying tissue. Fillers placed at the supraperiosteal level can compensate for this loss, restoring projection and support.
- Fat pad atrophy and descent: The malar fat pad, buccal fat, and periorbital fat all deflate and shift downward. This creates hollowing under the eyes, flattening of the cheeks, and deepening of the nasolabial folds. Treating these compartments directly, rather than filling the folds they create, produces more natural and longer-lasting results.
- Ligament laxity: The retaining ligaments of the face, including the zygomatic and masseteric ligaments, loosen over time. This allows soft tissue to descend, contributing to jowling and deepened facial contours.
- Muscle imbalance: Repeated muscle contractions over decades create dynamic wrinkles in the forehead, glabella, and periorbital region. Neuromodulators address this directly by reducing muscle activity at specific injection sites.
The following table summarises how aging changes each layer and the corresponding injectable approach:
| Facial layer | Age-related change | Injectable strategy |
|---|---|---|
| Bone | Resorption reduces projection | Deep supraperiosteal filler for structural support |
| Fat compartments | Atrophy and descent | Targeted volumisation of deflated compartments |
| Ligaments | Laxity allows tissue descent | Indirect support through volume restoration |
| Muscle | Hyperactivity creates dynamic lines | Neuromodulators (Botox, Nucieva, Xeomin) |
| Skin | Collagen loss, thinning | Superficial hydration fillers, skin treatments |
Many clients at Enrichedmedspa begin noticing these changes in their late 30s or early 40s, though some start preventive neuromodulator treatments in their late 20s to slow the development of deep dynamic lines. Starting earlier does not mean using more product. It means using less product more strategically, before structural changes become pronounced.
Key takeaways
Safe, natural-looking injectable results depend entirely on the practitioner’s depth of anatomical knowledge across all five facial layers, not on product volume alone.
| Point | Details |
|---|---|
| Five-layer anatomy guides placement | Each layer from skin to periosteum requires a specific injection depth and product type. |
| Danger zones require specialised technique | Glabella, nose, temples, and midface carry vascular and nerve risks managed through cannulas and micro-aliquots. |
| Natural results come from structural planning | Treating bone loss, fat compartment descent, and muscle activity together produces harmony, not isolated line correction. |
| Aging changes every layer simultaneously | Injectable plans must address bone resorption, fat atrophy, ligament laxity, and muscle imbalance as a whole. |
| Product selection must match anatomy | Filler firmness and cohesivity should correspond to the anatomical layer and tissue characteristics of each zone. |
Why anatomical knowledge is the standard, not a bonus
I have seen the difference that anatomical precision makes, and it is not subtle. Clients who have had treatments elsewhere often come in describing results they could not explain: a heaviness under the eyes, a flatness to the cheeks, or a stiffness that made them look tired rather than refreshed. In almost every case, the issue traces back to product placed in the wrong layer or the wrong zone, not too much product or the wrong product entirely.
The conversation around injectables has shifted significantly. The “refreshed, not frozen” standard that clients now expect is only achievable when the injector understands the interplay between muscle function, fat compartment position, and bony support. Expert injectors employ full facial assessment and anatomical mapping before every treatment, and this approach reduces complications while producing results that hold up over time.
What I find clients often misunderstand is that natural-looking results are not about using less product. Aging involves fat pad shifts, bone loss, and ligament laxity, and treating these holistically sometimes requires meaningful volume restoration. The difference between a result that looks natural and one that looks overdone is almost always placement, not quantity. Choosing a practitioner who prioritises ongoing anatomical education and a thorough pre-treatment assessment is the single most important decision you can make before any injectable treatment.
— Felix
Anatomy-based injectables at Enriched Med Spa
At Enrichedmedspa, every injectable consultation begins with a thorough assessment of your facial structure, including bony landmarks, fat compartment volume, and muscle activity patterns. This is not a formality. It is the clinical foundation that determines which products, depths, and techniques will produce the most natural result for your specific anatomy. Whether you are considering Botox or dermal fillers for the first time or refining a previous treatment, our team brings the anatomical training and product knowledge to guide you clearly. You can also explore our full range of dermal filler treatments to understand what is available and how each option aligns with your goals.
FAQ
What are the five layers of facial anatomy relevant to injectables?
The five layers are skin, hypodermis (subcutaneous fat), the SMAS, deep fat compartments, and the periosteum with underlying bone. Each layer requires a different injection depth and product type to achieve safe, natural results.
Why is the glabella considered a high-risk zone for fillers?
The glabella carries a high risk of vascular occlusion because the supratrochlear and supraorbital arteries run through this region. Filler injected here can compress or enter these vessels, potentially causing skin necrosis or, in rare cases, vision loss.
How does aging affect injectable treatment planning?
Age-related bone resorption, fat pad descent, ligament laxity, and muscle imbalance all change the structural context of the face. Effective injectable planning addresses these changes across multiple layers rather than treating surface lines in isolation.
What is the difference between a needle and a cannula for filler injections?
A needle is sharp and used for precise, targeted placement. A blunt-tip cannula is flexible and displaces vessels rather than puncturing them, making it the preferred tool in high-risk anatomical zones like the temples and midface.
How do I know if my injector has adequate anatomical training?
A well-trained injector will conduct a thorough facial assessment before treatment, explain which anatomical layer they are targeting, and discuss why specific products and techniques suit your anatomy. Ongoing facial anatomy training and continuing education are markers of a practitioner committed to safe, evidence-based practice.





